Задача
Изучить риск иммуноопосредованных воспалительных заболеваний (IMIDs) у пациентов с анкилозирующим спондилитом (AS)
Методы
Используя запрошенные данные за 2003-2012 гг. из Тайваньской национальной базы данных исследований в области медицинского страхования, мы выявили 30911 впервые диагностированных пациентов с АС, нуждающихся в медикаментозном лечении, с 2006 по 2012 г. Кроме того, мы случайным образом отобрали 309110 человек, не страдающих АС, которые соответствовали (1:10) пациентам с АС с учётом возраста, пола и года указателя даты.
После исключения субъектов с соответствующими предыдущими иммуноопосредованными воспалительными заболеванияи мы вычислили уровни заболеваемости (IR) различных IMID в когортах AS и не-AS и оценили коэффициенты риска (HR) с 95% доверительными интервалами после поправки на возраст, пол, Чарльсон-индекс сопутствующей патологии, частоту амбулаторных посещений в течение периода наблюдения и приёма лекарств. Мы провели анализ чувствительности, исключив тех, у кого иммунноопосредованное заболевание развилось в течение 3 месяцев от даты выборки.
Результаты
В последующем мы выявили, что у впервые диагностированных пациентов с АС значительно повышен риск развития острого переднего увеита, псориаза, синдрома Шегрена, облитерирующего тромбоангиита, болезни Бехчета и саркоидоза. Тем не менее, риск синдрома Шегрена не увеличился у пациентов с АС при анализе чувствительности.
В то же время, это исследование не выявило существенных различий в риске болезни Крона, язвенного колита, системной красной волчанки, системного склероза, дерматомиозита, полимиозита, пузырчатки и витилиго среди впервые диагностированных пациентов с АС и лицами без АС. Пациенты с AS имели значительно сниженный риск ревматоидного артрита.
Заключение
У тайваньских пациентов с впервые установленными диагнозами АС повышен риск развития острого переднего увеита, псориаза, облитерирующего тромбоангиита, болезни Бехчета и саркоидоза, но при этом снижен риск развития ревматоидного артрита.
Hsin-Hua Chen, Wen-Cheng Chao, Yi-Hsing Chen, Tsu-Yi Hsieh, Kuo-Lung Lai, Yi-Ming Chen, Wei-Ting Hung, Ching-Tsai Lin, Chih-Wei Tseng, Ching-Heng Lin
Arthritis Research & Therapy 2019 Aug 29; 21 (1): 196
DOI: 10.1186/s13075-019-1980-1
![]()
Risk of immune-mediated inflammatory diseases in newly diagnosed ankylosing spondylitispatients: a population-based matched cohort study
OBJECTIVE:
To investigate the risk of immune-mediated inflammatory diseases (IMIDs) in patients with ankylosing spondylitis (AS).
METHODS:
Using 2003-2012 claims data from the Taiwanese National Health Insurance Research Database, we identified 30,911 newly diagnosed AS patients requiring medical therapy from 2006 to 2012. In addition, we randomly selected 309,110 non-AS individuals matching (1:10) the AS patients with regard to age, sex and the year of the index date.
After excluding subjects with the corresponding prior IMIDs, we calculated the incidence rates (IRs) of various IMIDs in the AS and non-AS cohorts and estimated the hazard ratios (HRs) with 95% confidence intervals after adjusting for age, sex, the Charlson comorbidity index, the frequency of ambulatory visits during the follow-up period and medications. We conducted sensitivity analyses by excluding those who developed IMIDs within 3 months after the index date.
RESULTS:
In the follow-up period, we found that newly diagnosed AS patients had significantly increased risks of acute anterior uveitis, psoriasis, Sjögren’s syndrome, thromboangiitis obliterans, Behcet’s disease and sarcoidosis. However, the risk of Sjögren’s syndrome did not increase in AS patients in the sensitivity analysis.
In the same period, this study found no significant differences in the risks of Crohn’s disease, ulcerative colitis, systemic lupus erythematosus, systemic sclerosis, dermatomyositis, polymyositis, pemphigus and vitiligo between newly diagnosed AS patients and non-AS individuals. AS patients had a significantly reduced risk of rheumatoid arthritis.
CONCLUSION:
Newly diagnosed Taiwanese AS patients had increased risks of acute anterior uveitis, psoriasis, thromboangiitis obliterans, Behcet’s disease and sarcoidosis, but a reduced risk of rheumatoid arthritis.
Table 1 Demographic data and clinical characteristics of the study subjects
Таблица 1. Демографические данные и клинические характеристики субъектов исследования
| Non-AS | AS | ||
| (n = 309,110) | (n = 30,911) | P value | |
| Age, years (mean ± SD) | 42 ± 17 | 42 ± 17 | 1.00 |
| Sex | 1.00 | ||
| Female | 114,560 (37.1) | 11,456 (37.1) | |
| Male | 194,550 (62.9) | 19,455 (62.9) | |
| CCI (mean ± SD) | 0.22 ± 0.74 | 0.35 ± 0.89 | < 0.01 |
| CCI group | < 0.01 | ||
| 0 | 269,864 (87.3) | 24,208 (78.3) | |
| ≥ 1 | 39,246 (12.7) | 6703 (21.7) | |
| Prior IMID | |||
| Acute anterior uveitis | 604 (0.194) | 1695 (5.483) | < 0.01 |
| Psoriasis | 1019 (0.330) | 455 (1.472) | < 0.01 |
| Inflammatory bowel disease | 71 (0.023) | 18 (0.058) | < 0.01 |
| Crohn’s disease | 41 (0.013) | 7 (0.023) | 0.19 |
| Ulcerative colitis | 38 (0.012) | 13 (0.042) | < 0.01 |
| Systemic lupus erythematosus | 193 (0.062) | 79 (0.256) | < 0.01 |
| Sjögren’s syndrome | 137 (0.044) | 99 (0.320) | < 0.01 |
| Rheumatoid arthritis | 401 (0.13) | 345 (1.116) | < 0.01 |
| Systemic sclerosis | 20 (0.006) | 10 (0.032) | < 0.01 |
| Dermatomyositis | 12 (0.004) | 7 (0.023) | < 0.01 |
| Polymyositis | 11 (0.004) | 1 (0.003) | 0.93 |
| Thromboangiitis obliterans | 1 (0.0003) | 1 (0.003) | < 0.01 |
| Behcet’s disease | 18 (0.006) | 24 (0.078) | < 0.01 |
| Pemphigus | 16 (0.005) | 2 (0.006) | 0.77 |
| Sarcoidosis | 13 (0.004) | 6 (0.019) | < 0.01 |
| Vitiligo | 144 (0.047) | 30 (0.097) | < 0.01 |
- Data are presented as number (%) unless specified otherwise.
- Abbreviations: AS — ankylosing spondylitis, SD — standard deviation, CCI — Charlson comorbidity index, IMID — immune-mediated inflammatory disease.
- Данные представлены в виде относительной величины (%), если не указано иное.
- Сокращения: AS — анкилозирующий спондилит, SD — стандартное отклонение, CCI — индекс коморбидности Charlson, IMID — иммуноопосредованное воспалительное заболевание.
Table 2 Comparison of the incidence rates of developing various immune-mediated inflammatory diseases between AS patients and non-AS individuals
Таблица 2. Сравнение показателей заболеваемости развитием различных иммуноопосредованных воспалительных заболеваний у пациентов с АС и лиц без АС
| Autoimmune disease | Total | Event (%) | Total person-years | Incidence rate (/105 years) |
IRR (95% CI) |
| Acute anterior uveitis | |||||
| Non-AS | 307,265 | 420 (0.14) | 1,233,168 | 34.1 | Reference |
| AS | 28,335 | 643 (2.13) | 103,487 | 583.6 | 17.14 (15.13–19.41) |
| Psoriasis | |||||
| Non-AS | 307,048 | 508 (0.17) | 1,231,732 | 41.2 | Reference |
| AS | 30,240 | 176 (0.58) | 111,703 | 157.6 | 3.82 (3.22–4.53) |
| Inflammatory bowel disease | |||||
| Non-AS | 299,243 | 12 (0.004) | 1,205,603 | 1.0 | Reference |
| AS | 29,462 | 9 (0.03) | 109,791 | 8.2 | 8.24 (3.47–19.55) |
| Crohn’s disease | |||||
| Non-AS | 299,776 | 4 (0.001) | 1,207,612 | 0.3 | Reference |
| AS | 29,560 | 3 (0.01) | 110,132 | 2.7 | 8.22 (1.84–36.75) |
| Ulcerative colitis | |||||
| Non-AS | 308,500 | 8 (0.003) | 1,238,652 | 0.6 | Reference |
| AS | 30,793 | 7 (0.02) | 114,074 | 6.1 | 9.50 (3.45–26.20) |
| Systemic lupus erythematosus | |||||
| Non-AS | 308,500 | 40 (0.01) | 1,238,580 | 3.2 | Reference |
| AS | 30,517 | 29 (0.10) | 113,090 | 25.6 | 88.20 (11.03–705.18) |
| Sjögren’s syndrome | |||||
| Non-AS | 306,049 | 80 (0.03) | 1,230,358 | 6.5 | Reference |
| AS | 29,772 | 91 (0.31) | 110,650 | 82.2 | 12.65 (9.37–17.08) |
| Rheumatoid arthritis | |||||
| Non-AS | 305,326 | 112 (0.04) | 1,226,848 | 9.1 | Reference |
| AS | 27,531 | 190 (0.69) | 102,233 | 185.9 | 20.36 (16.12–25.71) |
| Systemic sclerosis | |||||
| Non-AS | 309,048 | 9 (0.003) | 1,240,674 | 0.7 | Reference |
| AS | 30,872 | 8 (0.03) | 114,346 | 7.0 | 9.64 (3.72–25.00) |
| Dermatomyositis | |||||
| Non-AS | 308,846 | 8 (0.003) | 1,239,911 | 0.6 | Reference |
| AS | 30,843 | 4 (0.01) | 114,233 | 3.5 | 5.43 (1.63–18.02) |
| Polymyositis | |||||
| Non-AS | 308,832 | 2 (0.001) | 1,239,818 | 0.2 | Reference |
| AS | 30,827 | 2 (0.01) | 114,166 | 1.8 | 10.86 (1.53–77.10) |
| Thromboangiitis obliterans | |||||
| Non-AS | 309,093 | 2 (0.001) | 1,240,854 | 0.2 | Reference |
| AS | 30,907 | 3 (0.01) | 114,474 | 2.6 | 16.26 (2.72–97.31) |
| Behcet’s disease | |||||
| Non-AS | 309,039 | 4 (0.001) | 1,240,654 | 0.3 | Reference |
| AS | 30,820 | 21 (0.07) | 114,144 | 18.4 | 57.06 (19.59–166.24) |
| Pemphigus | |||||
| Non-AS | 309,061 | 4 (0.001) | 1,240,728 | 0.3 | Reference |
| AS | 30,906 | 2 (0.01) | 114,477 | 1.7 | 5.42 (0.99–29.59) |
| Sarcoidosis | |||||
| Non-AS | 309,088 | 21 (0.01) | 1,240,775 | 1.7 | Reference |
| AS | 30,897 | 16 (0.05) | 114,402 | 14.0 | 8.26 (4.31–15.84) |
| Vitiligo | |||||
| Non-AS | 308,750 | 98 (0.03) | 1,239,523 | 7.9 | Reference |
| AS | 30,838 | 21 (0.07) | 114,251 | 18.4 | 2.32 (1.45–3.72) |
Abbreviations: AS — ankylosing spondylitis, IRR — incidence rate ratio, CI — confidence interval.
Сокращения: AS анкилозирующий спондилит, IRR — коэффициент заболеваемости, CI — доверительный интервал.
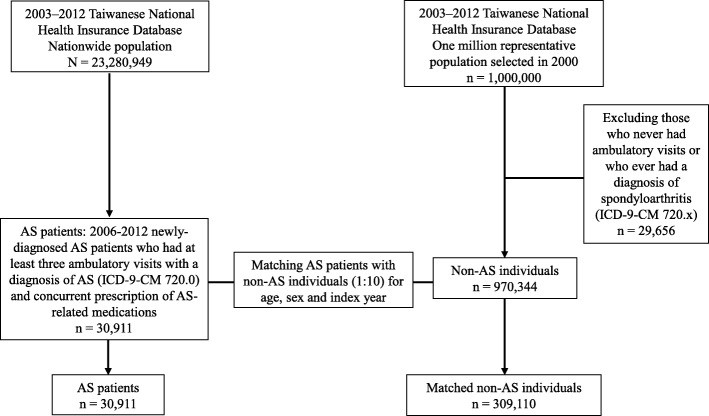
Fig. 1 Flow chart of study subject enrollment
Рис. 1. Блок-схема исследования и учёта данных.

![[Клинические характеристики больных подагрой с различным индексом массы тела]](https://rheumanews.ru/wp-content/uploads/2017/07/Zhonghua-nei-ke-za-zhi-Chinese-journal-of-internal-medicine-150x150-300x330.jpg)