Задача
Обновить научно-обоснованные рекомендации по лечению пациентов с анкилозирующим спондилитом (AS) и рентген-негативным аксиальным спондилоартритом (SpA).
Методы
Мы провели обновленные систематические обзоры литературы по 20 клиническим вопросам фармакотерапии, рассмотренных в руководствах 2015 года, и по 26 новым вопросам фармакотерапии, стратегии достижения цели и применения визуализации. Новые вопросы касались использования биоаналогов секукинумаба, икэкизумаба, тофацитиниба, ингибиторов фактора некроза опухоли (TNFi), а также снижения активности терапии биопрепаратами. Мы использовали методологию классификации рекомендаций, оценки, развития и методологию качественной оценки доказательств и формулирования рекомендаций с обязательным не менее 70% одобрением членов комиссии для голосования.
Результаты
Рекомендации по AS и рентген-негативному аксиальному SpA аналогичны. Ингибиторы ФНО рекомендуются по сравнению с секукинумабом или икекизумабом в качестве первого биологического препарата, который будет использоваться. Секукинумаб или изекизумаб более предпочтительны, чем использование второго TNFi у пациентов с первичным отсутствием ответа на первый TNFi. TNFi, секукинумаб и икекизумаб предпочтительнее тофацитиниба.
Совместное введение низких доз метотрексата с TNFi не рекомендуется. Также не существует строгой стратегии лечения или назначения, прекращения или снижения активности биологической терапии у пациентов со стабильным заболеванием. Сульфасалазин рекомендуется только при персистирующем периферическом артрите, когда TNFi противопоказан. Для пациентов с неясной активностью заболевания магнитно-резонансная томография позвоночника или таза может помочь в оценке. Регулярный мониторинг рентгенографических изменений с помощью серийных рентгенограмм позвоночника не рекомендуется.
Заключение
Эти рекомендации представляют обновленное руководство относительно использования новых лекарств и визуализации осевого скелета при лечении AS и рентген-негативного аксиального SpA.
Michael M. Ward, Atul Deodhar, Lianne S. Gensler, Maureen Dubreuil, David Yu, Muhammad Asim Khan, Nigil Haroon, David Borenstein, Runsheng Wang, Ann Biehl, Meika A. Fang, Grant Louie, Vikas Majithia, Bernard Ng, Rosemary Bigham, Michael Pianin, Amit Aakash Shah, Nancy Sullivan, Marat Turgunbaev, Jeff Oristaglio, Amy Turner, Walter P. Maksymowych and Liron Caplan
Arthritis Care & Research Vol. 0, No. 0, 2019 Aug 22, pp 1-15
DOI: 10.1002/art.41042
![]()
2019 Update of the American College of Rheumatology/Spondylitis Association of America/Spondyloarthritis Research and Treatment Network Recommendations for the Treatment of Ankylosing Spondylitis and Nonradiographic Axial Spondyloarthritis.
OBJECTIVE:
To update evidence-based recommendations for the treatment of patients with ankylosing spondylitis (AS) and nonradiographic axial spondyloarthritis (SpA).
METHODS:
We conducted updated systematic literature reviews for 20 clinical questions on pharmacologic treatment addressed in the 2015 guidelines, and for 26 new questions on pharmacologic treatment, treat-to-target strategy, and use of imaging. New questions addressed the use of secukinumab, ixekizumab, tofacitinib, tumor necrosis factor inhibitor (TNFi) biosimilars, and biologic tapering/discontinuation, among others. We used the Grading of Recommendations, Assessment, Development and Evaluation methodology to assess the quality of evidence and formulate recommendations and required at least 70% agreement among the voting panel.
RESULTS:
Recommendations for AS and nonradiographic axial SpA are similar. TNFi are recommended over secukinumab or ixekizumab as the first biologic to be used. Secukinumab or ixekizumab is recommended over the use of a second TNFi in patients with primary nonresponse to the first TNFi. TNFi, secukinumab, and ixekizumab are favored over tofacitinib.
Co-administration of low-dose methotrexate with TNFi is not recommended, nor is a strict treat-to-target strategy or discontinuation or tapering of biologics in patients with stable disease. Sulfasalazine is recommended only for persistent peripheral arthritis when TNFi are contraindicated. For patients with unclear disease activity, spine or pelvis magnetic resonance imaging could aid assessment. Routine monitoring of radiographic changes with serial spine radiographs is not recommended.
CONCLUSION:
These recommendations provide updated guidance regarding use of new medications and imaging of the axial skeleton in the management of AS and nonradiographic axial SpA.
Table 1. Definitions of key termsa
Таблица 1. Определения ключевых терминов
|
Term |
Definition |
|
Active disease |
Disease causing symptoms at an unacceptably bothersome level to the patient and judged by the examining clinician to be due to inflammation. |
|
Stable disease |
Disease that was asymptomatic or causing symptoms but at an acceptable level as reported by the patient. A minimum of 6 months was required to qualify as clinically stable. |
|
Primary nonresponse |
Absence of a clinically meaningful improvement in disease activity over the 3 to 6 months after treatment initiation, not related to toxicity or poor adherence. |
|
Secondary nonresponse |
Recurrence of ankylosing spondylitis activity, not due to treatment interruption or poor adherence, after having a sustained clinically meaningful improvement on treatment (generally, beyond the initial 6 months of treatment). |
|
Conventional synthetic antirheumatic drug |
Sulfasalazine, methotrexate, leflunomide, apremilast, thalidomide, pamidronate. |
|
Biosimilar |
Biopharmaceuticals that are copies of an original biologic medication and tested to be of the same purity and potency as the original. In these recommendations, we refer only to TNFi biosimilars. Examples include infliximab‐dyyb, etanercept‐szzs, and adalimumab‐atto. |
|
TNFi |
Infliximab, etanercept, adalimumab, certolizumab, golimumab, and their biosimilars. |
|
TNFi monoclonal antibodies |
Infliximab, adalimumab, certolizumab, golimumab. |
|
Biologics |
TNFi, abatacept, rituximab, sarilumab, tocilizumab, ustekinumab. |
|
High‐quality evidence |
Studies that provide high confidence in the effect estimate, and new data from future studies are thought unlikely to change the effect. |
|
Moderate‐quality evidence |
Studies that provide confidence that the true effect is likely to be close to the estimate but could be substantially different. |
|
Low‐quality evidence |
Studies that provide limited confidence about the effect, and the true effect may be substantially different from the estimate. |
|
Very low‐quality evidence |
Studies that provide very little certainty about the effect, and the true effect may be quite different from the estimate. |
|
Strong recommendation |
Action should be favored in almost all patients, usually requiring high‐quality evidence, high confidence that future research will not alter the conclusion, AND an assessment that the desirable effects of the intervention outweigh the undesirable effects. Should not be taken to imply that the intervention has large clinical benefits. |
|
Conditional recommendation |
Action should be followed in only selected cases, often limited by low‐quality evidence, OR when the desirable and undesirable consequences of an intervention are more balanced, OR if patients’ preferences for the intervention are thought to vary widely. |
|
Patient preferences |
Beliefs and expectations regarding potential benefits and harms of treatment and how these relate to an individual’s goals for health and life. |
|
Shared decision‐making |
The process by which a patient and clinician arrive at an individualized treatment decision based on an understanding of the potential benefits and risks of available treatment options and of a patient’s values and preferences. |
• TNFi = tumor necrosis factor inhibitor.
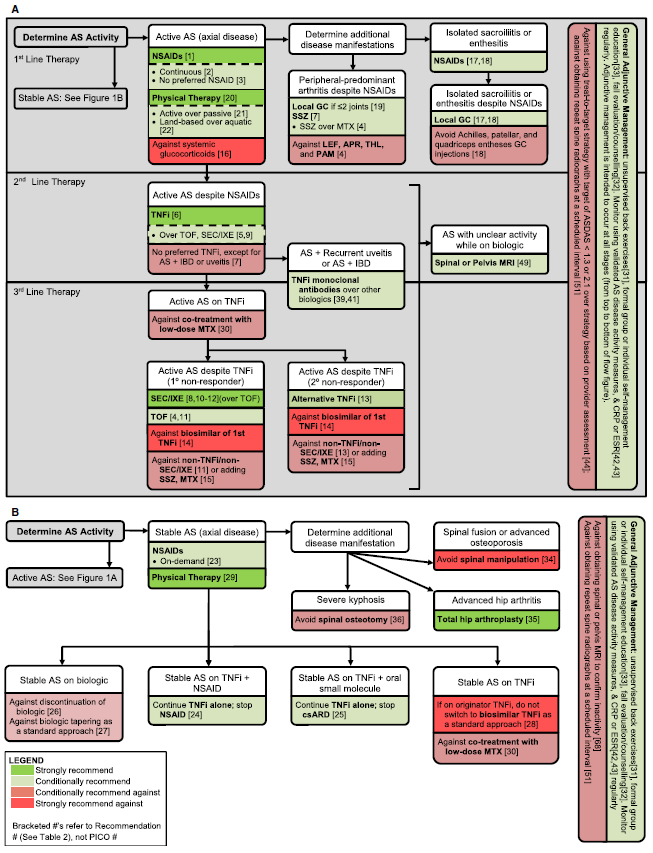
Рис. 1. Краткое изложение основных рекомендаций по лечению пациентов с активным анкилозирующим спондилитом (А) истабильным анкилозирующим спондилитом (В). AS = анкилозирующий спондилит; NSAIDs = нестероидные противовоспалительные препараты; GC = глюкокортикоид; SSZ = сульфасалазин; MTX = метотрексат; LEF = лефлуномид; APR = апремиласт; THL = талидомид; PAM = памидронат; TNFi = ингибитор фактора некроза опухоли; TOF = тофацитиниб; SEC = секукинумаб; IXE = икэкизумаб; IBD = воспалительное заболевание кишечника; csARD = обычные синтетические противоревматические препараты; ESR = скорость оседания эритроцитов; CRP = уровень С-реактивного белка; ASDAS = показатель активности болезни, вызванной анкилозирующим спондилитом; MRI = магнитно-резонансная томография; PICO = население, вмешательство, сравнение и результаты.
Figure 1. Summary of the main recommendations for the treatment of patients with A, active ankylosing spondylitis and B, stable ankylosing spondylitis. AS = ankylosing spondylitis; NSAIDs = nonsteroidal antiinflammatory drugs; GC = glucocorticoid; SSZ = sulfasalazine; MTX = methotrexate; LEF = leflunomide; APR = apremilast; THL = thalidomide; PAM = pamidronate; TNFi = tumor necrosis factor inhibitor; TOF = tofacitinib; SEC = secukinumab; IXE = ixekizumab; IBD = inflammatory bowel disease; csARD = conventional synthetic antirheumatic drugs; ESR = erythrocyte sedimentation rate; CRP = C- reactive protein level; ASDAS = Ankylosing Spondylitis Disease Activity Score; MRI = magnetic resonance imaging; PICO = population, intervention, comparison, and outcomes.